This year I was diagnosed with autism spectrum disorder (ASD)—alternatively known as autism spectrum condition (ASC). This diagnosis was not a surprise to me. In my head and heart, I have known for a long time—this was just the professional confirmation and validation I needed. I’m in my 30s now, and it pains me that my life could have been more successful had I been given this diagnosis in childhood. Sadly, a lack of awareness or education around the condition meant nobody ever identified my struggles, which led to me going without the support and understanding I so desperately needed until it was too late. Essentially, people assumed I was getting along just fine, so they decided that I wouldn’t need any support in life. Oh, how wrong they were.
Going back now to the end of 2008, when an acquaintance first pointed out that some of my traits were consistent with (what was formerly known as) Asperger syndrome, which is a neurodevelopmental disorder and form of autism. I had known somebody in high school who had this diagnosis but never attempted to learn anything about it. Upon researching it for myself, I suddenly felt overwhelmed with revelation—my entire life made sense for the first time. I could explain every little oddity, every difficulty and struggle. I could even explain my long-term mental health battles, of which countless psychologists had never been able to establish a root cause. It felt like I’d found the missing piece of the puzzle that was my life. I spent the following ten years trying (and failing) to convince medical professionals of the importance of an investigation. I saw it as a possible cause of—and hopefully solution for—all of the difficulties that they had been unsuccessfully treating. Unfortunately, they would all discredit my pleas with various disheartening responses. I’m sure many others diagnosed as autistic in adulthood can relate to the invalidating comments I would hear:
- “You don’t look/act autistic.”
- “We’re all somewhere on the autistic spectrum.”
- “So what? We all feel like that sometimes. It’s normal.”
- “Yes, you may be autistic, but we have to look at how reaching a diagnosis would change anything—how can we move forward without that?”
- “I think all men are autistic; it’s why they don’t understand what women really mean when they say they’re fine.”
- “I know somebody autistic, and you’re nothing like them.”
- “I think autism’s just made-up to excuse bad behaviour.”
- “You’re not autistic.”
- “Oh, I struggle with <one example difficulty> too—maybe I’m autistic as well!”
- “But you seem so normal!”
There may have been supportive intentions, but comments like these only serve to invalidate the difficulties that have destroyed mine and many other peoples lives. These difficulties are so much more than just an occasional minor annoyance that everybody experiences from time to time—this is constant, powerful, debilitating distress and disruption throughout your entire life. Perhaps I never stressed the strength of these difficulties to people enough, which is apt because some of the diagnostic criteria focus on difficulty explaining your feelings and experiences. I was determined and felt I owed it to myself to pursue this lead in search of answers, explanations, support and validation.
In 2018, I saw a new GP who had a vested interest in mental health, and I was delighted to finally be listened to by someone who recognised how important this was to me. I was referred for an adult autism assessment and was told at the time that there was an incredibly long waiting list of roughly a year on the NHS. Still, what’s an extra year on the decade I’ve already waited? Little did I know that I would eventually wait just over three-and-a-half years from the point of referral to eventual assessment (with no thanks to a particular global pandemic delaying things by an additional year). Honestly, I think if I’d known it would take that long to receive answers, I’d have saved up a couple of grand and paid to go private instead—but that’s hindsight for you.

So, what exactly is autism? The term originated in 1908 with psychiatrist Eugen Bleuler describing a subset of schizophrenic patients who were especially withdrawn and self-absorbed. This term was developed further in 1943 by child psychiatrist Leo Kanner, who described 11 intelligent children who had “a powerful desire for aloneness” and “an obsessive insistence on persistent sameness”. In 1944 scientist Hans Asperger described a milder form of autism. It wasn’t until 1977 that research showed autism was caused by genetics and biological differences in brain development. Autism is a spectrum condition where people share specific difficulties but are affected in different ways. It falls under an umbrella term coined in 1998—neurodiversity—divergence in mental or neurological function from what is considered typical or ‘normal’. Examples of other neurodivergent conditions are attention deficit hyperactivity disorder, dyslexia, dyscalculia, dyspraxia, Tourette syndrome, acquired brain injury and other learning disabilities.
Some reports have suggested that as much as 1-2% of the UK population is autistic. This number has risen over the decades—not because the condition is becoming more prevalent, but because as time progresses, awareness and education are making the signs easier to spot, which means more people get referred for diagnosis. Thus the percentage of diagnoses given is higher as a result of a larger sample of referrals. Many people can go their entire lives undiagnosed, having no idea that they are neurodivergent—some of them get by in life just fine, and others struggle without knowing why.

Autism’s theory of causation is incomplete, but experts generally accept that it develops during pregnancy and birth. The signs become apparent sometime before a child is three years old (i.e. when they develop socially and intellectually). Autism cannot be created or cured by vaccination or medical treatment—it’s more akin to having a specific eye colour—you’re born with it, it’s with you for life, it’s often genetic and is part of who you are. For example, a few years ago, my cousin in Sydney received an adult autism and ADHD diagnosis—and when I think of the grandfather we both share, I wouldn’t be surprised if some of his traits placed him on the spectrum too.
It’s important to point out that repeatedly exposing an autistic person to their difficulties will never make those difficulties easier for them—it will only cause unnecessary distress and trauma. The key to a happy life is to find alternative methods and coping mechanisms. On the flip side, some autistic people may find individual strengths in their condition. Some examples of neurodivergent strengths are:
- organisation skills
- an ability to absorb and recall large amounts of information
- precision
- reliability
- ability to hyper-focus on tasks
- an ability to look at situations from a different viewpoint
- independence
- self-motivation
- detail-oriented
- extreme honesty
- unbiased opinions
- fair and just
One charity—The National Autistic Society—splits its description of common autistic difficulties into six sections:
- Social communication and social interaction challenges
- Repetitive and restrictive behaviour
- Over- or under-sensitivity to light, sound, taste or touch
- Highly focused interests or hobbies
- Extreme anxiety
- Meltdowns and shutdowns
From what I’ve experienced, it seems many people have an idea in their heads of what autism is and are often surprised when they learn more about it. Whilst their preconceived notion of autism isn’t necessarily inaccurate, it’s usually just one extreme they are thinking of—in fact, the spectrum is immensely diverse. In 2013 multiple conditions were folded into the ASD/ASC label. The spectrum now contains three levels ranked according to severity, ranging from Level 1 (“high-functioning” individuals requiring support) to Level 3 (“low-functioning” individuals requiring very substantial support). Whilst my diagnosis report doesn’t specify a level, I assume I would fall under Level 1, which is roughly equivalent to what used to be referred to as Asperger syndrome (before the controversy surrounding Hans Asperger became more well-known). The terms “high-functioning” and “low-functioning” are generally frowned upon within the autistic community; they are considered harmful, demeaning and don’t reasonably consider a person’s strengths and capabilities—instead, these terms measure an autistic individual’s needs by how their condition affects other people. There has been significant progress in raising awareness of the autism spectrum, but there is still a long way to go.
Whilst the process might be different for other providers and countries, my assessment experience consisted of the following elements:
- An initial interview questionnaire to establish the main reasons for assessment and outline the sort of challenges I face daily.
- A developmental history telephone interview between an occupational therapist and my mum (as somebody who has known me best since birth). My mum was worried that she would have forgotten crucial information or missed key details from my upbringing, but it seems what she could contribute was sufficient. Following the interview, there was an online questionnaire for gathering further information.
- An ADOS-2 (autism diagnostic observation schedule, second edition) video call with two highly specialised speech and language therapists who had intentionally not read any previous information about me—this was their first impression. This call consisted of an informal chat followed by three small ‘play’ tasks, with the therapists observing my natural mannerisms, behaviours and responses. The three tasks involved talking the therapists through an everyday exercise, telling the story from a textless children’s picture book and making up my own story using small props. This assessment should have been carried out face-to-face; however, they have had to adapt to a virtual alternative for global pandemic reasons.
- This was an unrequired element, but I sent them a 10-page document I’d been working on for the past 13 years. Every time I’d remember something that could prove relevant, I’d add it to the list. It turns out it was beneficial for the detailed specifics but only served to confirm what they had already established from their evidence. Nevertheless, the final report included my input.
- A multi-disciplinary team meeting that I was not present for, where the speech and language therapists combine all collected evidence and present it to a larger team, including senior clinical psychologists who have leads in autism. The diagnostic criteria they were assessing me on is from the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), used in many countries to define all aspects of mental health.
- A first feedback appointment. I was given the diagnosis and informed that all of the professionals involved in the assessment unanimously agreed that I was autistic. I learned that it’s rare the team are all in agreement so quickly, as generally, at least one of them will have doubts. I found this immensely reassuring, as I often feel like a fraud on the few occasions where something goes right for me—a form of imposter syndrome, I suppose.
- A diagnosis report. They compiled a 20-page report explaining the findings which led them to their decision. There are a few little bits where they appear to have misinterpreted the specifics of something I’ve said, but it’s only trivial details and not worth asking them to correct.
- A second feedback appointment. This is to give me a chance to process the diagnosis and ask any questions that may have arisen.
I found the whole process stressful—but at the same time, I was surprised at how relaxed and informal it all was. Everybody involved seemed lovely, which certainly helped, compared to other medical assessments I’ve participated in in the past that felt more like police interrogations. I’d never taken part in a substantial video call before, as that is something I am incredibly uncomfortable with. I can’t say I’ll be rushing to do it again!
In that moment, during the first feedback appointment, when the therapist finally delivered the diagnosis, I felt ambivalent emotions. On the one hand, I felt massive relief that my long battle was finally over. I felt pride that I had fought through to the end and received the outcome I needed. The answers I had sought for over a decade were finally here. On the other hand, I immediately started doubting them, thinking they could have got it wrong because things never run so smoothly for me. But of course, it’s not a mistake—it can’t be—how would little-old me be able to fool an entire group of highly qualified and specialised medical professionals? Perhaps it’s still sinking in, but that’s a very typical response from me—if I won the lottery, I’d probably ask if they’ve made a mistake.

During my long wait for assessment, I chose not to discuss my ‘self-diagnosis’ with people (other than a select few and an online support group) out of fear that I could be wrong and have to backtrack shamefully. I just needed it to be official first. Last year, in the aftermath of a series of distressing incidents, the clinical psychologist I was seeing urged me to seek out a sunflower lanyard (which discreetly indicates hidden disabilities to members of the public who are aware of the scheme). Even then, I felt like a fraud wearing it before I’d received a proper diagnosis, despite having other conditions that would satisfy the criteria for use. Additionally, many selfish people have been abusing the lanyard scheme during the pandemic which has reduced public trust in it. Don’t get me started on those shameful human beings who have stolen that chance of dignity from disabled people. I suppose I’m just somebody who worries a lot about what people think of me—which ties in with my habit of masking and creating a persona that I think people will like.

In my mother’s interview, she noted that I was a very observant child and regularly noticed small changes or details. Examples include a random house we’d walk past every day adding a horseshoe above their garage door, spelling mistakes on posters, or a TV show changing the font used in their end credits. I barely spoke until I was 3 or 4 and had a limited vocabulary, mostly just noises and a small selection of words, but I absorbed all of the information around me. I was timid and enjoyed reading books from my meticulously organised bookshelf. I loved writing my own stories. I would speak very quietly and use little eye contact. I would miss sarcasm and take everything literally (for example, “You’re driving me up the wall!” baffled me because I didn’t have a car and couldn’t drive, let alone vertically up a wall). I preferred to spend time alone in my own little world just getting on with my special interests—many of which would be considered niche, such as car number plates or floorplans. My reception teacher would call on me to fix the BBC Micro computer in the classroom whenever it ‘broke’. I would cry and break down when things got too much for me, even in my teens when it was less socially acceptable to do so. On some particularly overwhelming occasions, I would have meltdowns—way beyond your average child’s temper tantrum. One I always remember was during a rare weekend in my grandparents’ care, where they wanted to spontaneously take me to a “fun” kids’ restaurant, Charlie Chalk’s, which wasn’t part of the ‘itinerary’. More commonly, however, I would just quietly shut down and behave as if I was on auto-pilot.
I was a child who didn’t know how to tell people what was wrong, and I would ‘mask’ without realising I was masking, so I can’t blame anybody for not picking up on the signs earlier. They were well hidden, and nobody asked the necessary questions. Any difficulties were always explained away by things like moving house, grieving or simply being sensitive. If I were growing up in the 2020s, I believe there would have been more chance of a school teacher or doctor recognising patterns and traits thanks to better training and awareness of autism. Perhaps it could have saved me a lifetime of pain.

I spoke previously about how I’ve struggled terribly with my mental health since childhood. I was medicated and put through various therapies from 13 onwards, which never really helped and landed me with a treatment-resistant depression diagnosis by 2014. I’d wondered for a long time if these difficulties have always been caused by toiling with an underlying autism spectrum condition, which has a common link with mental health struggles. If the professionals had approached my problems from the wrong angle all those years, it could explain why the various therapies have essentially been a waste of time and resources. Is this why I’m now a broken 30-something with no idea who I am, always feeling like an alien among my peers? Is this why I feel shame every time I get something wrong or try to over-compensate in every interaction, suffering perpetual exhaustion from the crazy and confusing expectations the world has of me? These are the questions I needed to answer.

In that recent post mentioned above I wrote about how I ‘lie’ to everybody around me by masking my true self, my feelings and putting on a fake persona to survive each day, particularly in social situations. I mentioned “other issues”, which I said I would talk about in the future. This is those “other issues”, which I can finally discuss with certainty and is the true reason for the masking behaviours that exhaust me so much.
I was planning on writing about some of the most significant difficulties I face in adulthood because one of the reasons I’m taking the time to talk about this is to open up about my personal experience. Having given it some thought, I feel those specifics should remain private. Additionally, I’d hate to inadvertently make something so severe for me sound trivial to everybody else because autism goes a lot deeper than just being shy, sensitive, quirky or disliking sensations. In addition to the debilitating aspects of autism, my diagnosis conveniently explains curious little traits that confused my loved ones over the years—like niche interests and obsessions or how I often connect better with dogs than humans.
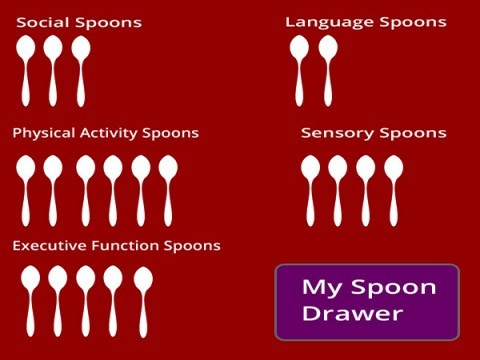
What I will say is that Spoon Theory is very much applicable. This term is a metaphor developed by Christine Miserandino (in her case to express how it felt to have lupus) used to describe the amount of mental or physical energy a person has available for daily activities and tasks, with each of these tasks using up ‘spoons’. The theory is an excellent way to explain why some days you can cope better with certain events than others and how you can plan to ensure you have ‘spoons’ left to get you through to the end of the day. I prefer to use a battery level metaphor, perhaps a percentage or number of bars that quickly deplete throughout the day. If you do a battery-intensive task first thing in the morning, it’s going to affect how you respond to and reserve your battery for other tasks for the rest of your day. If you run out of battery, you’re going to shut down. In times of continually heightened stress like the COVID-19 pandemic, it’s like you’re starting each day on half capacity.
Something I find fascinating is that, because of my many years of mental health treatment, psychology has become somewhat of a special interest of mine. I suppose I’ve trained myself to pick up on certain social cues via this interest rather than an instinct that is ‘impaired’ through autism. I use this interest in my fiction, and I’ve learned to recognise good use of psychology with character development in TV and film. The problem is, I don’t know if I’m doing it correctly—for all I know, I’ve got it all wrong, and nobody wants to be the one to correct me. Taking advantage of your strengths to make up for your shortcomings probably isn’t an uncommon trait for autistic people. I was so pleased to discover autistic YouTuber Adam Wonders—whom I strongly identify with and would recommend his content for an insight into my life—had pursued a career in psychology with a backstory very similar to my own.

I knew a diagnosis wouldn’t be some miracle fix for all my problems and didn’t expect that suddenly my quality of life would improve—it was always about understanding myself more than anything else. Diagnosis may ‘open a few doors’ for me support-wise, and my report signposted many self-help resources. I’ve even bought a book (see right) written from the perspective of somebody in my situation—although finding the concentration to absorb it will be a challenge! I have a lot of fear that my diagnosis may also close some metaphorical doors, but that’s for another post.
Without a diagnosis, I often struggled to explain my distress to people successfully—they’d think I was exaggerating, over-dramatising or being a hypochondriac and I’d receive little in the way of empathy. Now that I have a diagnosis, I can hopefully provide a bit of context to those struggles. The struggles, of course, are still perfectly valid even without a diagnosis.
Ultimately, I would like to say to anybody in a position like I was, where you feel you relate powerfully to criteria in a way strong enough that it makes sense of your life—don’t let anybody fob you off. This acknowledgement is essential. You need to know.

Perhaps you care for a child who you suspect may be neurodivergent, and their teachers and doctors keep telling you that they will get through life just fine without diagnosis or a statement of needs. Don’t give up on them. There may come a time in their future when they desperately need that support and have to put up an even bigger fight to receive it. Maybe you won’t be around to provide the developmental history that may prove crucial in their assessment. Do it while you can—and whilst they’re young—to give them the best opportunity for a happy, successful life where you can continue celebrating and embracing their differences. If they receive a diagnosis and it turns out they can get through their life just fine regardless, then that’s cool too—they don’t need to disclose their diagnosis to anybody if they choose not to, but it’s there if they need it. It’s a win-win situation.
Understanding that there is a cause and explanation for your difficulties is worth the diagnosis alone. Unlocking individualised and appropriate support is a bonus. I hope this will be the beginning of a better path for me. It’ll probably take time to undo all the damage, but hopefully, my future is looking a little bit brighter now.
Discover more from IAreSam
Subscribe to get the latest posts sent to your email.
[…] year I was diagnosed with an autism spectrum condition, and I wrote about some of my experiences until that point. My life is full of negatives, so today, I wanted to try and pull some positives […]
[…] year I was diagnosed with an autism spectrum condition, and I wrote about some of my experiences until that point. My life is full of negatives, so today, I wanted to try and pull some positives […]
[…] days, I’m less comfortable with telling people that I am diagnosed as autistic. I feel like autism awareness may have gone too far in the wrong direction, coupled with the rise […]
[…] daily life and those around you? What strategies can enhance your well-being? When I was formally diagnosed with autistic spectrum disorder a few years ago, I received an extensive reading list along with my […]
[…] variety. Looking back, I now realise this was likely a symptom of my (at the time) undiagnosed autism spectrum disorder. Even as an adult, my preference for bland, boring foods remains, and people have always made me […]